

Decision Intelligence 4 Health (di4h)
fyi …
See TEAM Public Health articles on being decisive.
For di4h decision modeling, visit: https://di4health.github.io
Visit Alliance for Decision Education, co-founded by Annie Duke.
See our latest di4h framework (figure below).
On this page we cover:
Decision making
Decision intelligence (DI)
Decision Intelligence 4 Health (DI4H)
Population health data science (PHDS)
Resources for DI/DI4H and PHDS
1 Decision making
Embedded in all journeys (life, learning, strategy, innovation, etc.) are the choices we make. Since medical school in the 1980s, when I was introduced to the nascent field “decision analysis,”1 I came to appreciate that decision making is our most important daily activity. Annie Duke says it best:2
“… there are only two things that determine how your life turns out: luck and the quality of your decisions. You have control over only one of those two things.”
“… your decision-making is the single most important thing you have control over that will help you achieve your goals.”
Annie Duke, How to Decide: Simple Tools for Making Better Choices. Penguin Publishing Group, 2020.
In spite of its importance, decision quality is rarely formally taught. This is a shame! Some of reasons include the complex, trans-disciplinary nature of descriptive and normative decision theories.
For starters, every decision involves
choices, causality, and prediction
outcomes, trade-offs, and opportunity costs
memory and sensory inputs
core beliefs and cognitive biases
emotions, reasoning, and actions
uncertainty and constraints
intuitive (“System 1”) vs deliberative (“System 2”) decisions3
first order vs second order4 decisions
individual vs. group (non-competing) decisions
single party vs multi-party (competing, interdependent)5 decisions
Every decision is influenced by one or more of the following:
values and/or goals
drives and/or impulses
stresses and/or pressures
faulty reasoning (eg, from VUCA)
learning and/or improvement opportunities
Finally, every decision has consequences (including unintentional, unseen, etc.).
Studying decisions holistically will pay off many times over in improving your life (personal, family, community, teams, and organizations) and your work. You will learn a ton and be able to apply the concepts daily! Studying decision quality is transformational and ensuring decision quality in team decisions is the basis for decisive leadership!
Studying decision quality is transformational and ensuring decision quality in team decisions is the basis for decisive leadership!
2 Decision intelligence (DI)
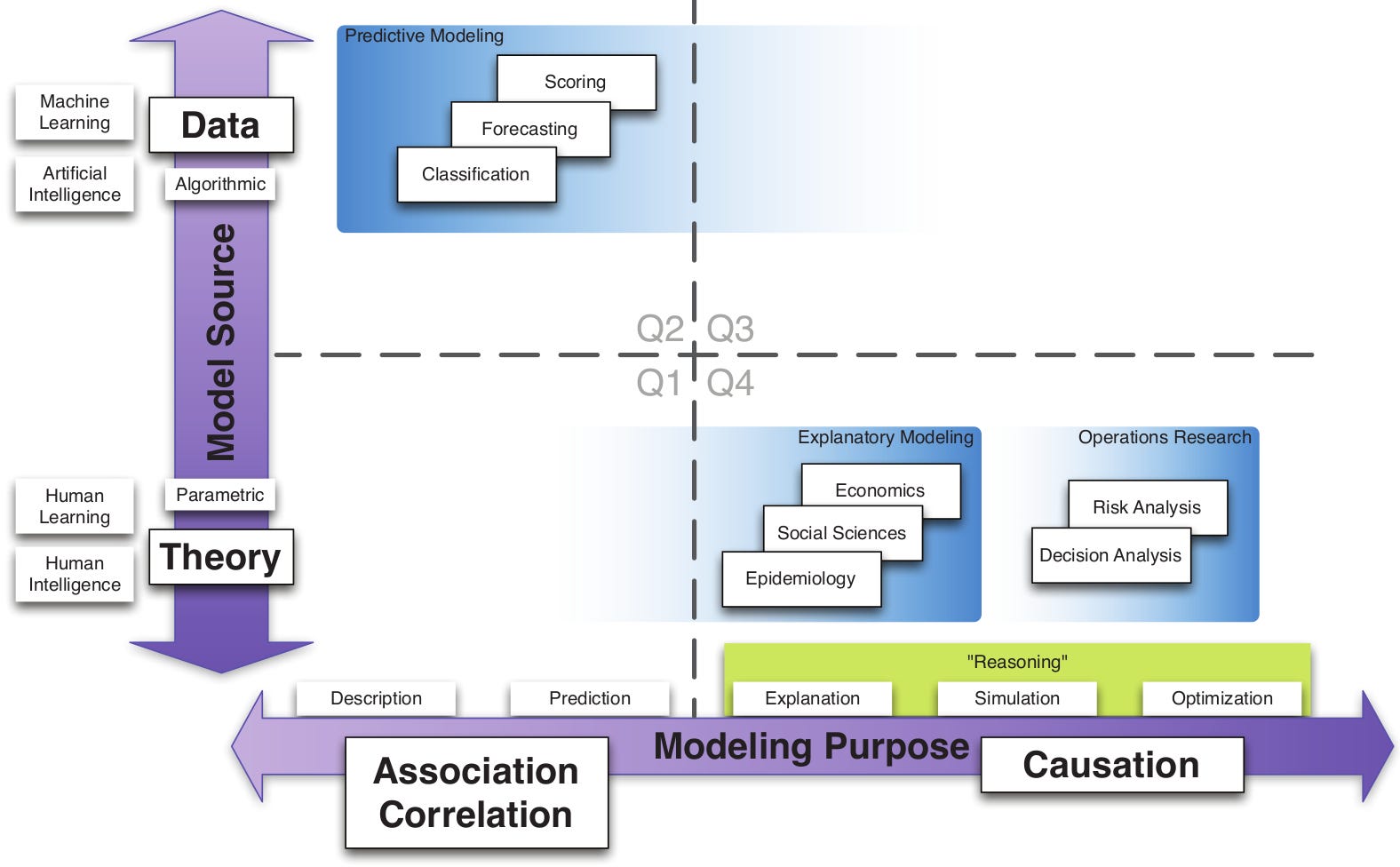
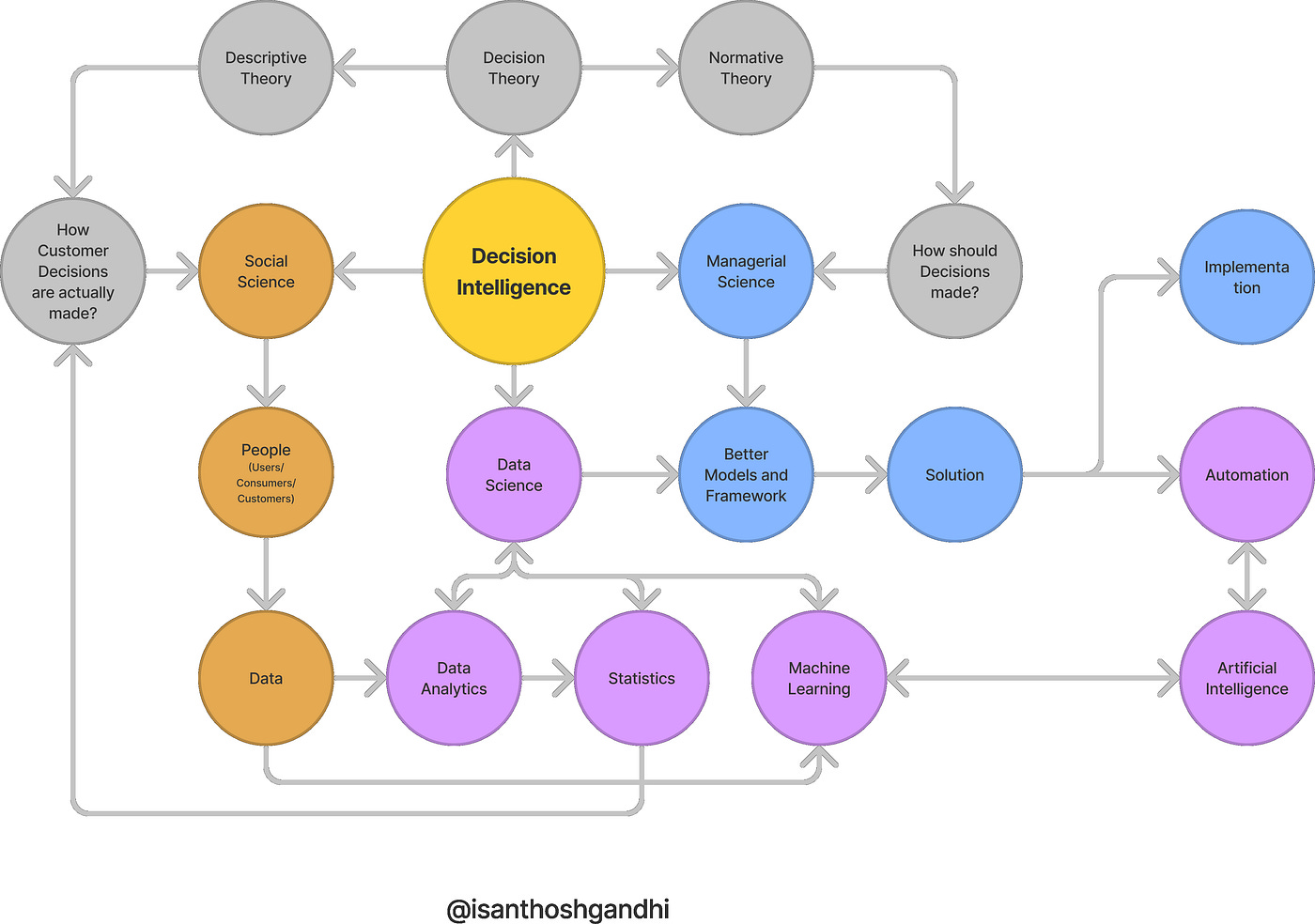
Formally, “decision intelligence is an engineering discipline that augments data science with theory from social science, decision theory, and management science”6 (Figure 1).

In industry, decision intelligence focuses on integrating automation, artificial intelligence, and data analytics to optimize business operations. For example, from Aera Technnology, key aspects of decision intelligence are the following:
Data-driven decisions: Uses real-time, historical, structured, and unstructured data to inform actions.
AI and automation: Applies logic and rules to automate decisions, reducing manual work and improving speed.
Context-aware intelligence: Considers business goals, constraints, and environments in each recommendation.
Scenario planning: Enables simulation of multiple outcomes to support smarter choices.
Continuous learning: Improves decision quality through feedback loops.
Decision intelligence repositions humans as decision architects who design how decisions are made. It operates at three levels of AI involvement, depending on the type of data:
Decision support (human in the loop): AI provides insights and performs simulations with alternative paths (eg, scenario modeling for pricing decisions)
Decision augmentation (human on the loop): AI provides recommendations with full context and possible impact, and a human makes the final call to execute, change or reject the decision (eg, recommendations for supplier sourcing)
Decision automation (human out of the loop): AI autonomously makes decisions and takes action within predefined constraints, with full auditability of actions (eg, fully executed logistics optimization).
Before public health professionals become “decision architects” as described above and here, first they need to become competent decision makers in the tactical and strategic decision challenges they face daily. Only then, will they be a strong position to adapt appropriately tech-driven decision intelligence.
For public health, the approach needs to be grounded in the realities of public health practice which differ significantly from industry, including health care.
3 Decision Intelligence 4 Health (DI4H)
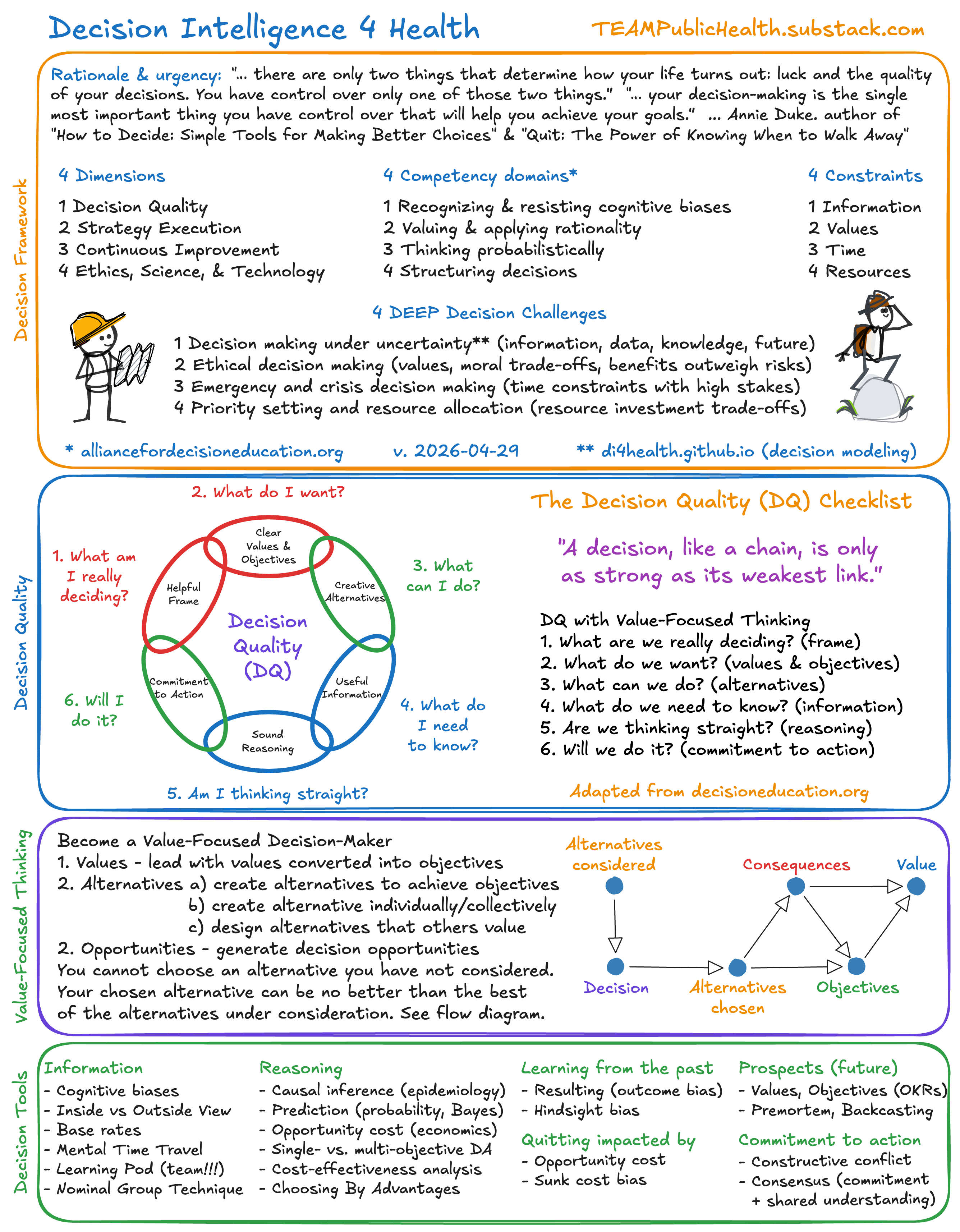
Decision Intelligence 4 Health (di4h) is using ethics, science, and technology to improve team decision-making in the face of constraints, challenges, and trade-offs.
Decision Intelligence 4 Health has
4 dimensions (Figure 2),
4 constraint types (information, values, time, and resources),
4 competency domains, and
4 DEEP decision challenges.
For more details see this slide presentation.
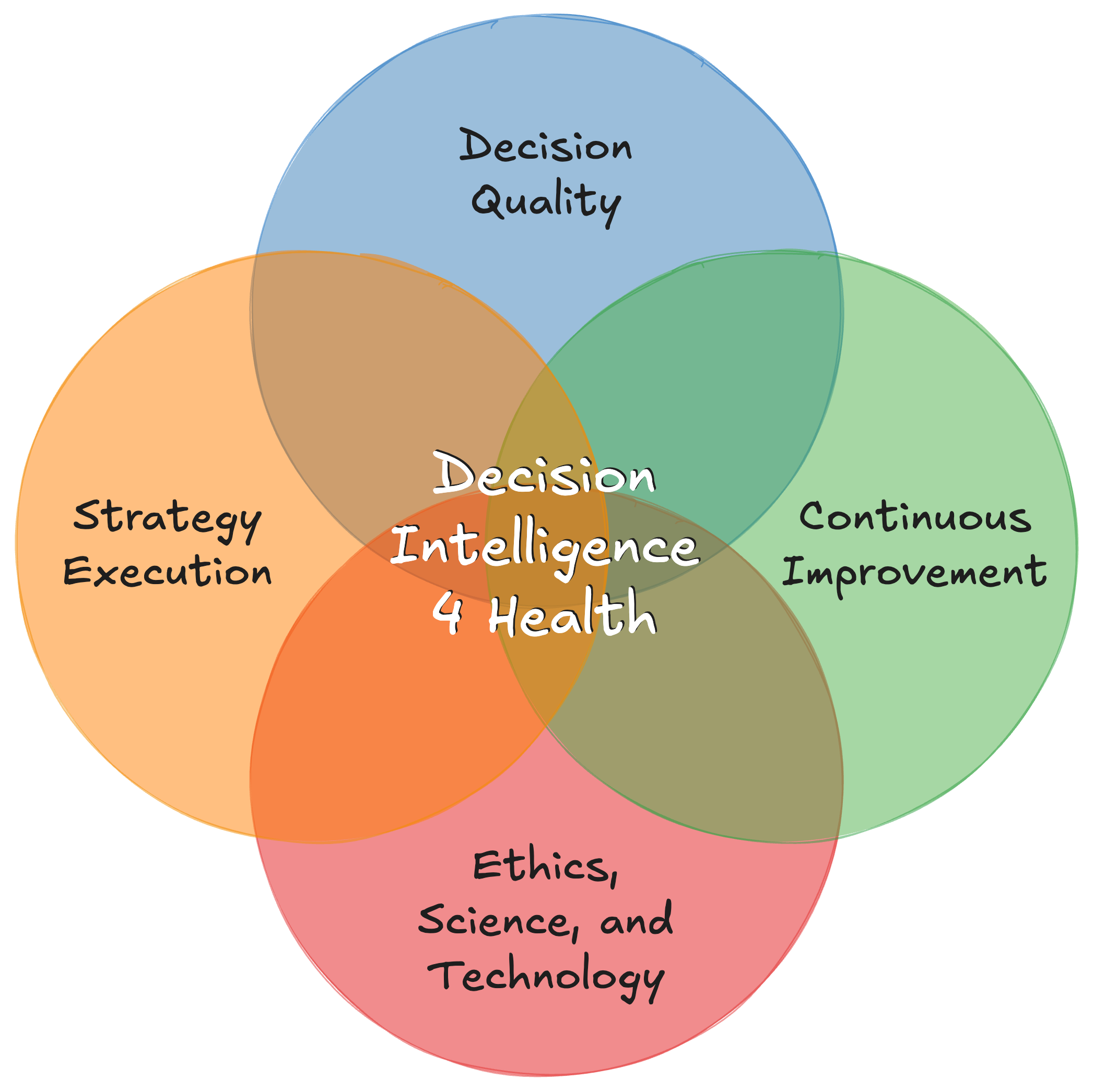
The DI4H 4 dimensions (Figure 2) with examples are
Decision Quality frameworks (our focus is DQ)
“Practical Wisdom”
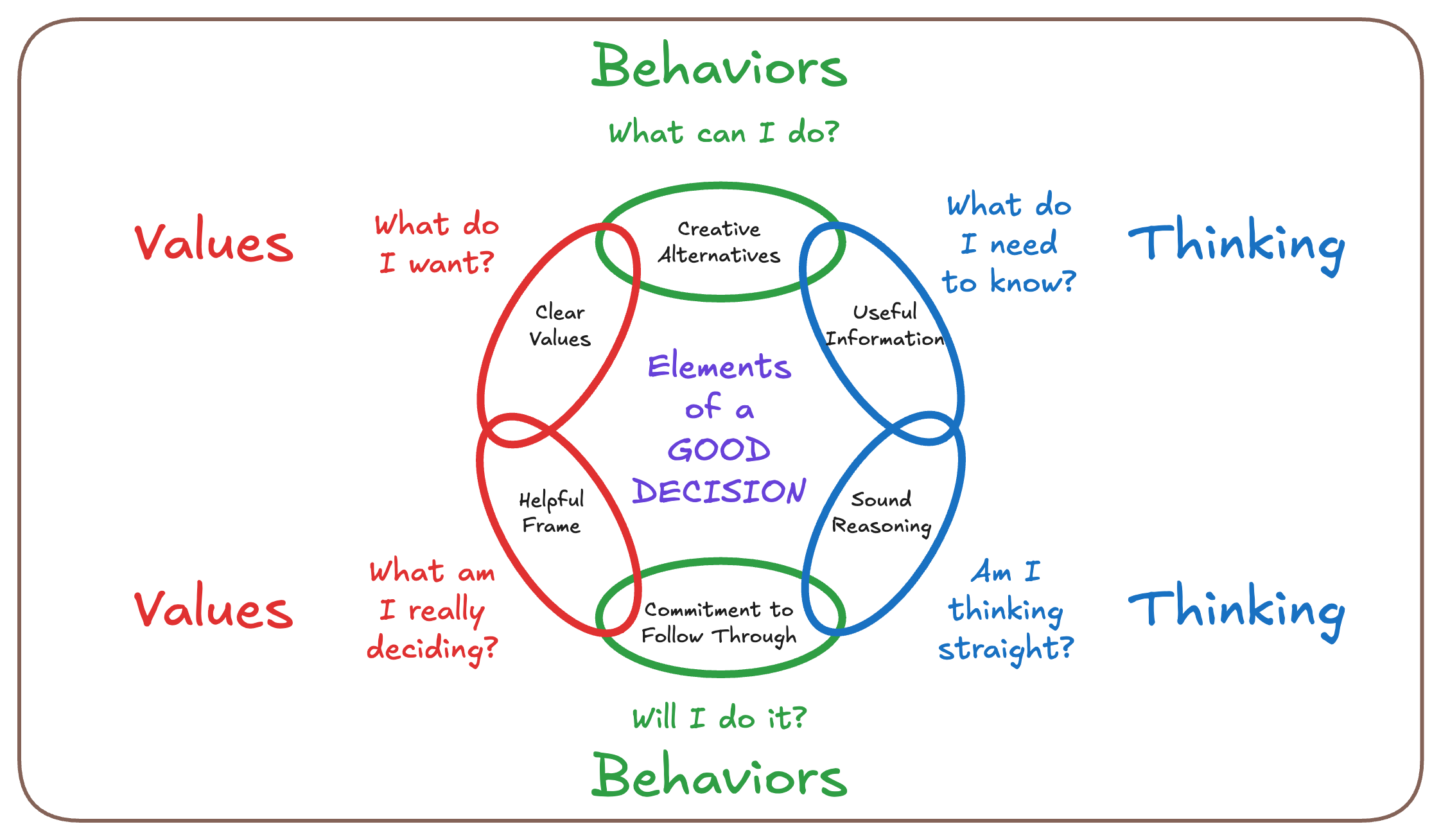
The Decision Quality (DQ) Checklist
Strategy Execution frameworks
Continuous Improvement frameworks
Design thinking (human-centered design)
Ethics, Science, and Technology
public health and medical ethics
psych, health econ, data science
computation and artificial intelligence
The DI4H 4 competency domains are
Recognizing and resisting cognitive biases
Valuing and applying rationality7
Thinking probabilistically
Structuring decisions (ie, DQ tool)
The 4 competency domains are from the Alliance for Decision Education.
And, the DI4H 4 DEEP decision challenges faced by health and human services organizations are
Decision making under uncertainty (information, data, knowledge, future)
Ethical decision making (moral trade-offs, benefits outweigh risks)
Emergency and crisis decision making (time constraints)
Priority setting and resource allocation (resource investment trade-offs)
Leaders and teams for health and human services organizations are confronted with these four DEEP decision challenges. These highlight important constraints: values, information, time, and resources. These categories are not mutually exclusive — they overlap! Health and human services organizations must master these DI4H DEEP decision challenges.
Decision Intelligence 4 Health (DI4H) is using ethics, science, and technology to improve strategic health decisions in the face of uncertainty, time constraints, and trade-offs.
An example using the Decision Quality Chain
The Decision Chain has six quality requirements (“links”):
What am I really deciding? (frame)
What do I want? (values)
What can I do? (alternatives)
What do I need to know? (information)
Am I thinking straight? (reasoning)
Will I do it? (commitment to action)
For more ideas on how to use the Decision Quality Chain, download this 24-page booklet from the Decision Education Foundation.
The elements of decision quality are always applied within a strategy execution or continuous improvement framework. I recommend starting with PDSA.
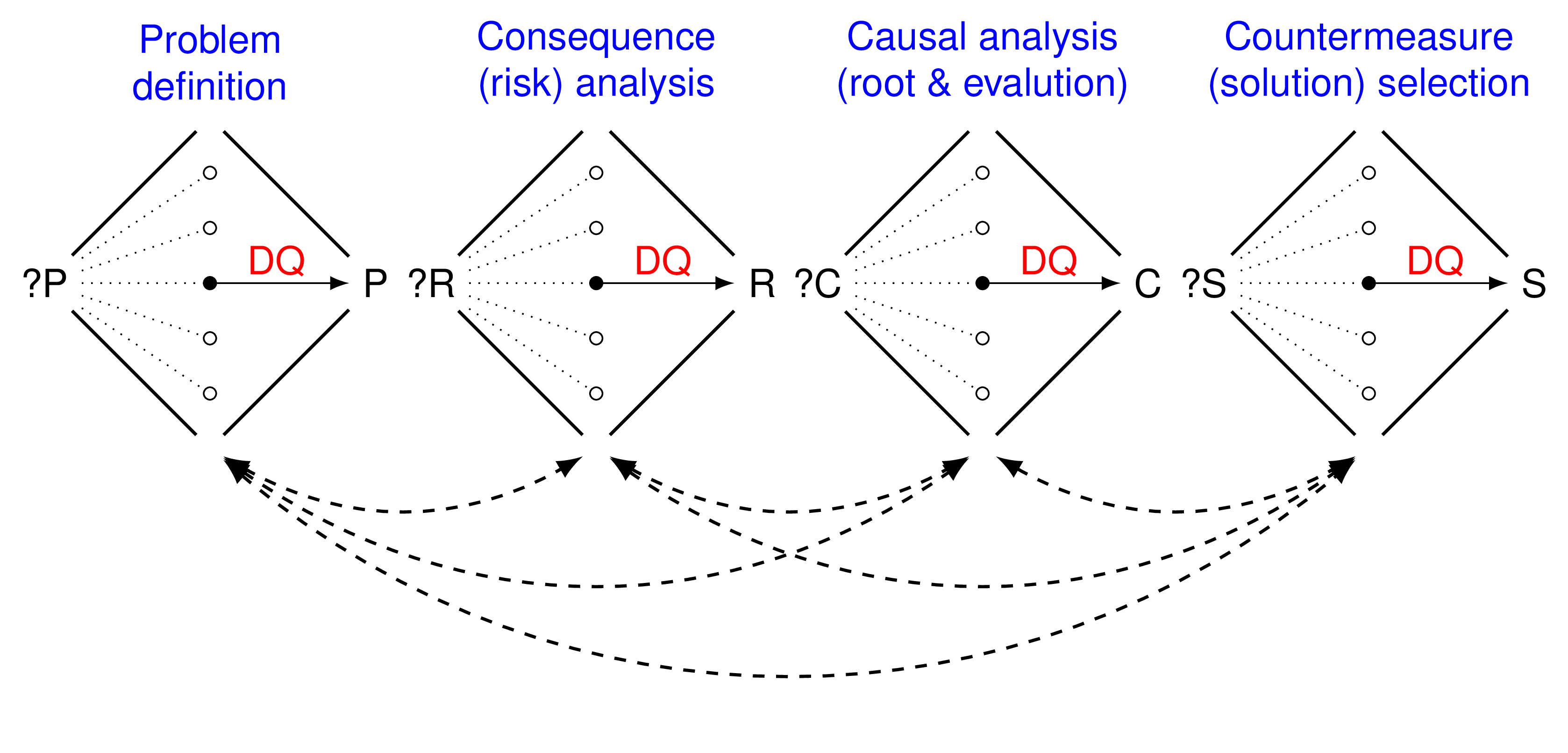
Figure 4 is a different view of the Decision Quality Chain.
Figure 5 and 6 depicts how it is actually used in practice. Figure 4 is PDSA problem solving as a causal graph.
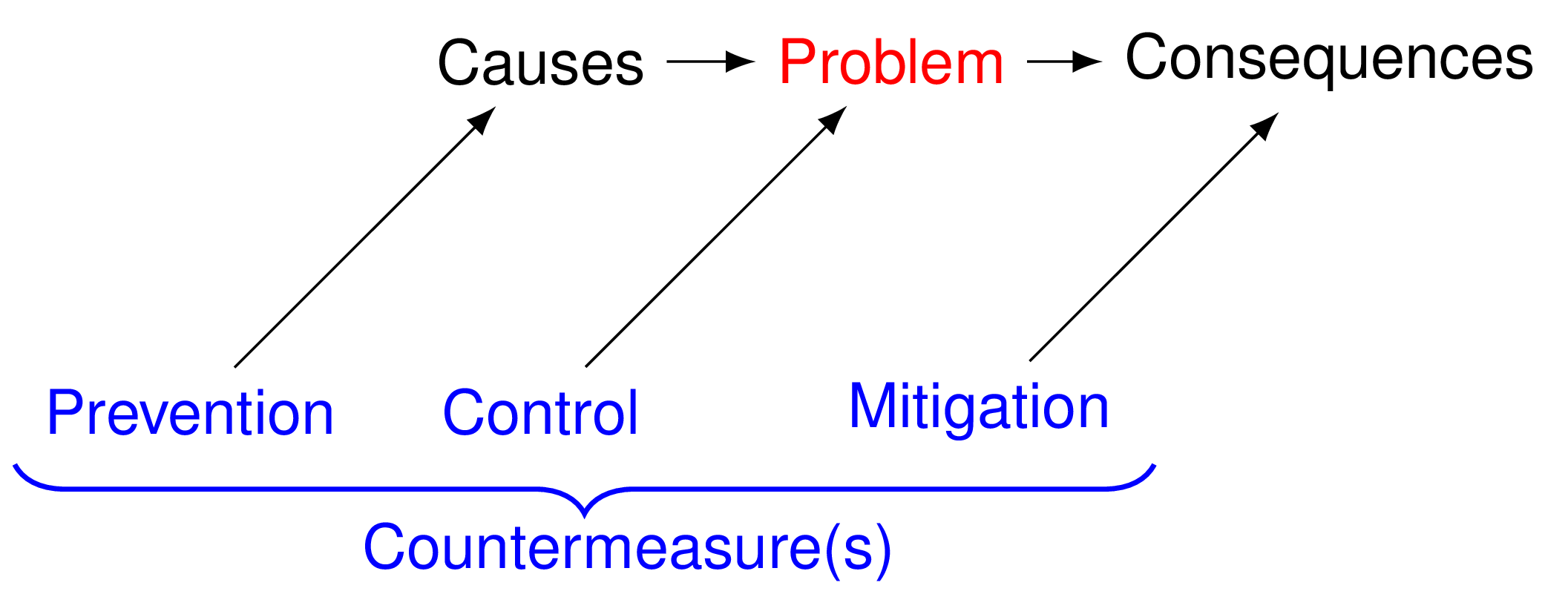
Figure 6 is a graphical depiction of the DQ Chain deployed within PDSA problem solving.
For more details, see this slide presentation or read this article:
Aragón, Tomás J., Sara H. Cody, Christopher Farnitano, et al. “Crisis Decision-Making at the Speed of COVID-19: Field Report on Issuing the First Regional Shelter-in-Place Orders in the United States.” Journal of Public Health Management and Practice 27, no. Supplement 1 (2021): S19–28. https://doi.org/10.1097/PHH.0000000000001292.
The elements of decision quality are always applied within a strategic execution or continuous improvement framework. I recommend starting with PDSA.
Data science (below) should be in service of decision intelligence (above).
4 Population Health Data science (PHDS)
For 15 years, I taught “Applied Epidemiology Using R” (2004-2019) at UC Berkeley School of Public Health. During that time I witnessed the emergence of “data science.” Data science is the multidisciplinary field of extracting insights and actionable knowledge from structured and unstructured data. This is actually backwards: values, goals, and decisions should drive data science.
In contrast, population health data science (PHDS) is the study of transforming data into knowledge and decisions that protect and improve the health and well-being of populations.
Population health data science is the study of transforming data into knowledge and decisions that protect and improve the health and well-being of populations.
On this page I will also post selected resources for population health data science (Figure 3) applied to decision intelligence for public health.8
PHDS has five levels (Table 1). Most organizations (including health organizations) are at Level 1 (description) and, sometimes, Level 2 (prediction). Level 3 (explanation) is implementing modern causal inference methods. Level 4 (simulation) is mathematical modeling for epidemiological or decision insights (eg, CDPH CalCAT). Level 5 (optimization) is seeking to optimize decision, effectiveness, or efficiency metrics. Familiar examples include decision analysis, cost-effectiveness analysis, and cost-benefit analysis. Less familiar to public health are methods from management science (aka, operations research), Bayesian networks, machine learning, and artificial intelligence. Decision intelligence operates on PHDS Level 5 and builds on concepts and methods from all levels.
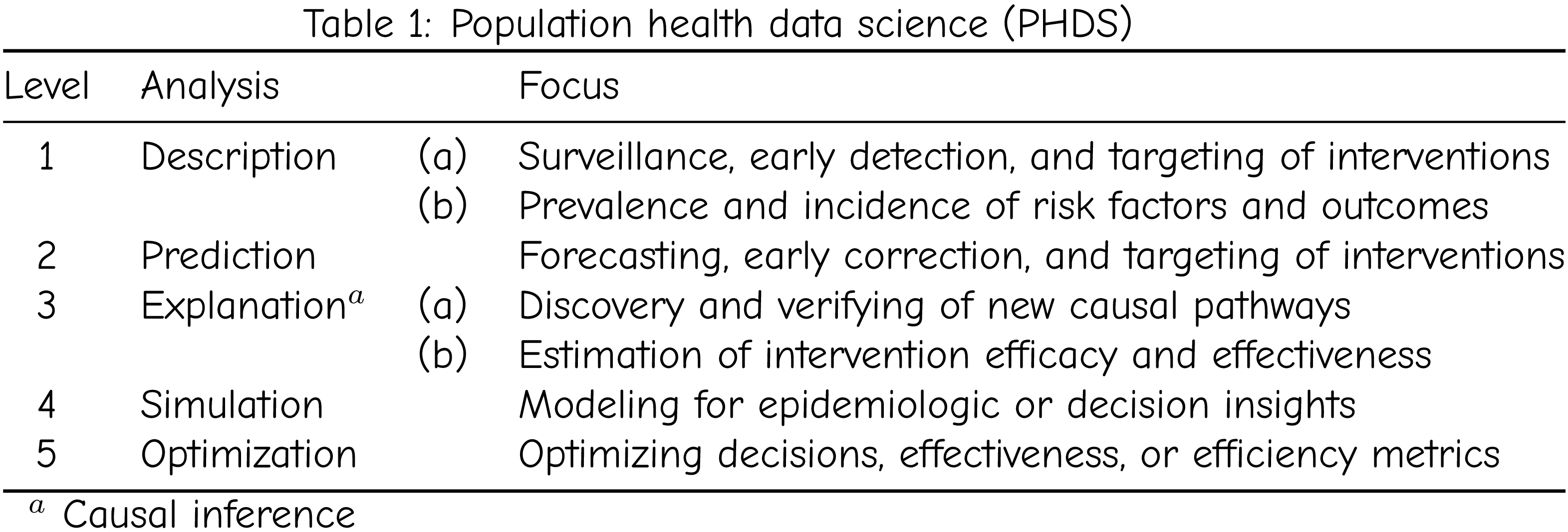
Decision intelligence operates on PHDS Level 5 and builds on concepts and methods from all levels.
Resources
Resources for Decision Intelligence 4 Health
Alliance for Decision Education (foundation)
Decision Education Foundation (foundation)
University of Texas at Austin Strategic Decision and Risk Management (executive education)
Harvard Center for Health Decision Science (academic)
RAND Corporation
Carnegie Mellon University AI Institute for Societal Decision Making (academic)
Computational resources for PHDS and DI4H
R language
R packages for decision intelligence
Julia language
Julia packages for decision intelligence
DecisionProgramming.jl (decision analysis with influence diagrams)
Bayesian networks
Markov Decision Processes
Python
pgmpy (causal inference and probabilistic inference using Directed Acyclic Graphs and Bayesian Networks)
Decision making software
The programming languages above can be use for decision making. For example, in this tutorial paper, “Population health thinking with Bayesian networks,” I demonstrate how to use R to conduct decision analysis. However, it is easier to use dedicated software. Here are some popular software solutions:
Appendix
Detailed view of Figure 1.
Appendix
Practical wisdom* for daily decision challenges of life and work
Step 1 – Start here (3 questions) for direction, commitment, and alignment. This step is often sufficient.
What are our values?
What are our goals?
What decisions will lead to outcomes that move us closer to our goals?
Step 2 – If you have time, do Step 2 (4 questions). Involve a team with cognitive diversity.
What are the worst outcomes and how will we avoid them? (pre-mortem) (ie, mental contrasting)
What are the best outcomes and how will we achieve them? (backcasting)
What new behaviors/activities do we need to start?
What old behaviors/activities do we need to stop?
Step 3 – This is the “last mile” of decision making – making decision stick!
How will we manage the powerful psychological processes (antecedents, core beliefs, cognitive biases, emotions, desires, drives, cravings, etc.) so that we make good decisions that stick!
*Inspired by Judy Ho, Annie Duke, and Stoic philosophy. See Tomás Aragón. “Public Health Practice as Stoicism in Action - How the Wisdom of Ancient Philosophers Shows up in Public Health Practice.” TEAM Public Health, December 28, 2025. https://teampublichealth.substack.com/p/public-health-practice-as-stoicism.
Footnotes
Weinstein, Milton C., and Harvey V. Fineberg. Clinical Decision Analysis. Saunders, 1980.
Duke, Annie. How to Decide: Simple Tools for Making Better Choices. Penguin Publishing Group, 2020. https://www.annieduke.com/books/.
“System 1 and System 2 thinking describes two distinct modes of cognitive processing introduced by Daniel Kahneman in his book Thinking, Fast and Slow. System 1 is fast, automatic, and intuitive, operating with little to no effort. This mode of thinking allows us to make quick decisions and judgments based on patterns and experiences. In contrast, System 2 is slow, deliberate, and conscious, requiring intentional effort. This type of thinking is used for complex problem-solving and analytical tasks where more thought and consideration are necessary.” Source: https://thedecisionlab.com/reference-guide/philosophy/system-1-and-system-2-thinking
Strategies or rules used to simplify or govern how you make multiple first-order decisions.
For example, as in game theory.
“Rationality” includes causal inference, systems thinking, understanding opportunity costs, etc.
In 2019, I started learning Python to complement R. When the COVID-19 pandemic struck, I stopped all teaching and coding. When I returned to coding, I discovered the Julia language! Julia is now my “go-to” language for scientific computing.